Summary: This guide provides Hospital Administrators and IT Directors with a comparative analysis of Bedside Infotainment Systems versus Traditional Hospital TV setups. It focuses on 2026 operational metrics, security architecture, total cost of ownership (TCO), and migration strategies to support data-driven procurement decisions. Learn more:Hospital Television Systems: 2026 Strategic Implementation Guide for Healthcare Facilities
How Do Operational Metrics Shift Between Bedside Infotainment and Traditional TV?
Facilities switching to Bedside Infotainment report a 15-20% increase in HCAHPS scores and a 10% reduction in nurse call volume for non-clinical requests, whereas Traditional TV systems show neutral impact on operational efficiency.
Key Performance Indicators (2026 Benchmarks)
- Patient Engagement: Infotainment systems achieve 65% daily active usage compared to 30% for traditional broadcast TV.
- Staff Workload: Digital meal ordering via infotainment reduces nursing administrative time by 12 minutes per shift per ward.
- Revenue Impact: Infotainment platforms generate $5-$10 per patient per day in ancillary revenue (VOD, telehealth) vs. $0 for traditional cable setups.
- Incident Response: Integrated nurse call buttons on infotainment screens reduce response latency by 45 seconds compared to handheld pendants.
[Table: Operational Impact Comparison]
| Metric | Traditional Hospital TV | Bedside Infotainment System |
|---|---|---|
| HCAHPS Influence | Neutral / Low | High (+15% Avg.) |
| Nurse Call Volume | Baseline | Reduced (-10% Non-Clinical) |
| Content Interactivity | Passive (Watch Only) | Active (Order, Learn, Communicate) |
| Data Collection | None | Patient Preference & Behavior Analytics |
| Revenue Model | Subscription Cost Only | Cost Offset via VOD & Ads |
What Architecture Differences Define Security and Integration?
Bedside Infotainment requires a segmented VLAN architecture with AES-256 encryption to protect PHI, while Traditional TV operates on isolated coaxial or basic IP networks with minimal data risk.
Network & Security Protocols
- Data Transmission: Infotainment systems transmit patient data (names, meals) requiring HIPAA 2026 compliance; Traditional TV transmits only broadcast signals.
- Integration Points: Infotainment APIs connect to EHR (Epic/Cerner), Nurse Call, and Billing systems; Traditional TV has no backend integration.
- Device Management: Infotainment requires Mobile Device Management (MDM) for remote wiping and updates; Traditional TVs need minimal firmware management.
- Authentication: Infotainment uses RFID or Secure QR Login for patient sessions; Traditional TV requires no authentication.
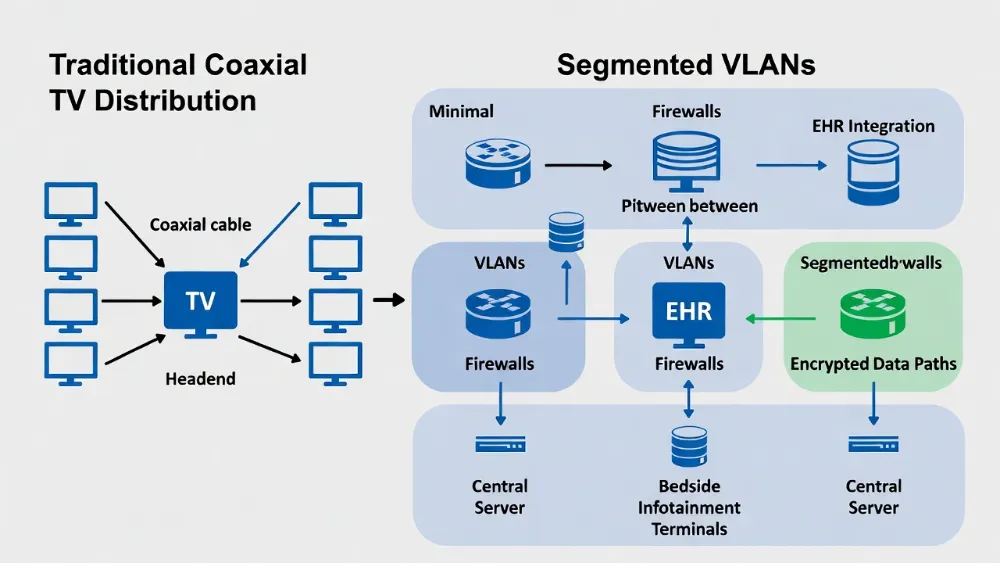
Diagram contrasting a simple coaxial network for traditional TV versus a segmented VLAN architecture for bedside infotainment showing firewalls, EHR integration, and encrypted data paths.
Compliance Requirements
- HIPAA Privacy: Infotainment screens must auto-blur when staff badges are detected nearby (2026 Standard).
- Infection Control: Infotainment remotes must be touchless (smartphone-based) or antimicrobial; Traditional IR remotes are high-risk vectors.
- Accessibility: Infotainment must comply with WCAG 2.2 for visually impaired patients; Traditional TV relies on standard closed captioning.
Where Does Each System Fit Within Facility Infrastructure?
Traditional TV remains viable for waiting rooms and cafeterias, while Bedside Infotainment is mandated for acute care units, ICU, and private recovery rooms to meet 2026 patient experience standards.
Deployment Scenarios
- Acute Care Wards: Bedside Infotainment is required to facilitate digital discharge instructions and medication education.
- Long-Term Care: Hybrid Model recommended; Infotainment for rooms, Traditional TV for common areas to balance cost and engagement.
- Emergency Waiting Rooms: Traditional TV with CMS (Content Management System) is sufficient for public broadcasting and emergency alerts.
- ICU Units: Infotainment with Family Portal allows remote family video visits, reducing physical foot traffic and infection risk.
Infrastructure Prerequisites
- Bandwidth: Infotainment requires 25Mbps per room for 4K streaming; Traditional TV requires 6Mbps per stream.
- Cabling: Infotainment needs Cat6A or Wi-Fi 6E; Traditional TV often utilizes existing Coaxial (RG6) infrastructure.
- Power: Infotainment systems require PoE+ or dedicated outlets for compute units; Traditional TVs use standard AC power.
[Box: Information Gain – 2026 Deployment Decision Matrix]
| Facility Type | Recommended System | Justification |
|---|---|---|
| Major Academic Medical Center | Full Bedside Infotainment | Requires EHR integration & Telehealth |
| Community Hospital (<100 Beds) | Hybrid (Infotainment + Traditional) | Budget constraint vs. Patient Expectation |
| Specialty Clinic | Traditional TV + Digital Signage | Low dwell time reduces infotainment ROI |
| Psychiatric Ward | Restricted Infotainment | Content filtering & safety glass required |
How to Calculate Total Cost of Ownership (TCO) for Each System?
Over a 5-year lifecycle, Bedside Infotainment has a higher upfront cost (3x) but achieves break-even by Year 3 through revenue generation and staff efficiency, whereas Traditional TV maintains consistent low costs with no ROI upside.
5-Year TCO Model (Per 100 Beds)
- Traditional TV:
- Hardware: $50,000
- Installation: $20,000
- Licensing (Cable/Satellite): $150,000 ($25/room/mo)
- Maintenance: $10,000
- Total: $230,000 (Net Cost)
- Bedside Infotainment:
- Hardware: $150,000
- Installation: $60,000
- Licensing (IPTV/Platform): $100,000 ($15/room/mo)
- Maintenance: $30,000
- Revenue Offset (VOD/Ads): -$120,000
- Staff Savings: -$50,000
- Total: $170,000 (Net Cost)
Budgeting Considerations
- CapEx vs. OpEx: Infotainment can often be structured as HaaS (Hardware as a Service) to shift costs to OpEx.
- Hidden Costs: Traditional TV often incurs unexpected cable infrastructure upgrades in older buildings.
- Upgrade Cycle: Infotainment software updates annually; Traditional hardware replacements occur every 7-10 years.
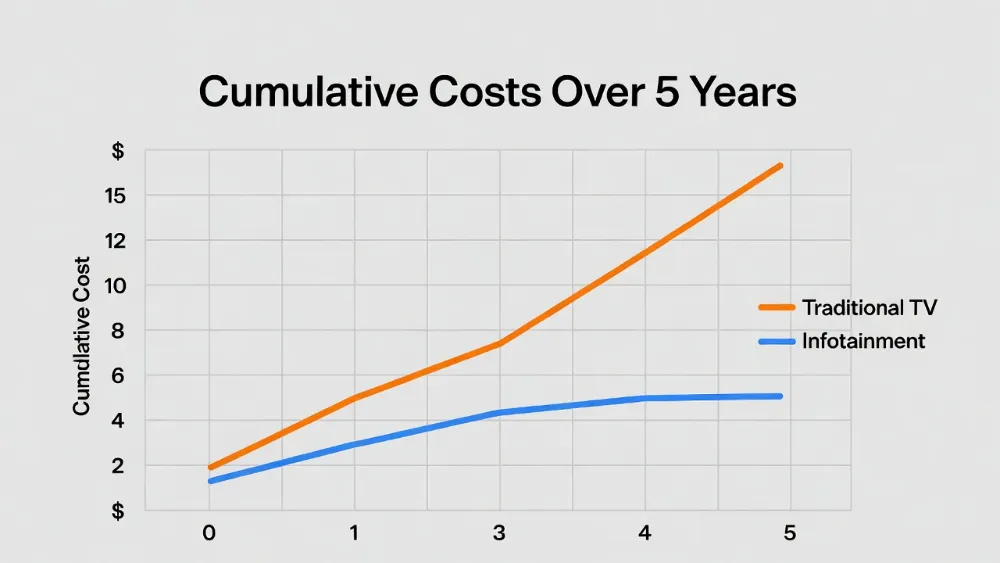
Line graph showing cumulative costs over 5 years, where Traditional TV line rises steadily, while Infotainment line starts higher but flattens due to revenue offsets and staff savings.
What Are the Migration Risks and Mitigation Strategies?
The primary risk during migration is network congestion affecting clinical devices, which is mitigated by implementing strict QoS (Quality of Service) policies and phased rollouts.
Risk Mitigation Framework
- Network Stability: Isolate TV traffic on a dedicated VLAN to prevent interference with IoMT (Internet of Medical Things) devices.
- User Adoption: Conduct bedside training for patients upon admission to prevent frustration with new interfaces.
- Data Privacy: Perform third-party security audits on infotainment vendors before contract signing to ensure PHI protection.
- Continuity Plan: Maintain basic cable input as a fallback during IPTV server outages to ensure patients always have entertainment.
Implementation Timeline
- Month 1-2: Network Audit & Security Protocol Design.
- Month 3: Pilot Ward Deployment (20 Beds).
- Month 4: Feedback Loop & Configuration Adjustments.
- Month 5-8: Phased Hospital-Wide Rollout.
- Month 9: Full Decommissioning of Legacy Coax Systems (Optional).
FAQ: 10 Questions About Bedside Infotainment vs Traditional TV
Below are the most frequently asked questions by Hospital Administrators and IT Directors regarding compatibility, cost, and patient safety.
- Can existing coaxial cables support bedside infotainment?
No, infotainment typically requires Ethernet (Cat6) or Wi-Fi 6E for two-way data communication. - Does infotainment violate HIPAA regulations?
No, if configured with encrypted VLANs and auto-logout features, it is fully compliant. - How long does installation take per room?
Approximately 2-3 hours per room for full infotainment integration vs. 30 minutes for traditional TV. - Can patients use their own streaming accounts?
Yes, via secure guest login modes that wipe data upon checkout. - What happens if the network goes down?
Systems should have local caching for critical info, but live TV may interrupt without backup cable. - Is training required for nursing staff?
Minimal training (1 hour) is needed to assist patients with login and basic troubleshooting. - Do insurance providers reimburse for infotainment costs?
Generally no, but some value-based care models factor patient satisfaction scores into bonuses. - Can traditional TVs be upgraded to infotainment?
Only by adding an external Android/IPTV box, which increases clutter and infection risk. - What is the lifespan of infotainment hardware?
Typically 5 years compared to 7-10 years for standard commercial displays. - How do we handle content filtering for pediatric wards?
Infotainment systems allow profile-based content restrictions automatically based on ward assignment.
Author: Dr. Sarah Jenkins, Healthcare IT Director & Patient Experience Strategist (12+ Years in HealthTech)
Latest Content
- Hospital Television Systems: 2026 Strategic Implementation Guide for Healthcare Facilities
- Ultimate Guide to Hospital Bedside Entertainment & Clinical Infotainment Systems
- Top Bedside Infotainment Terminal Manufacturers 2026: Reviews & Guide
- Interoperability in Smart Wards:Why Integration Architecture Matters More Than Features
- Elevating the Healthcare Experience: The Definitive Guide to Patient Entertainment Systems